The Soviet Union: Healthcare
[Part of the Soviet Union series]
In a previous post, I talked about Soviet GDP growth. In this post, I will discuss the healthcare system in the Soviet Union.
I went and looked for most of the papers written on soviet healthcare. Most, if not all of them present a negative view of the system. If you think I'm cherrypicking my evidence, because it's implausible that there are zero papers claiming the system worked relatively well, you can go to google scholar and search for such evidence. There were some people claiming that it worked Iwell in the 70s, but that was before the West had access to reliable data, and today no one considers those claims believable.
Here's what the Soviet Union promised its citizens:
Article 42. Citizens of the USSR have the right to health protection. This right is ensured by free, qualified medical care provided by state health institutions; by extension of the network of therapeutic and health-building institutions; by the development and improvement of safety and hygiene in industry; by carrying out broad prophylactic measures; by measures to improve the environment; by special care for the health of the rising generation, including prohibition of child labour, excluding the work done by children as part of the school curriculum; and by developing research to prevent and reduce the incidence of disease and ensure citizens a long and active life. (Soviet Constitution, 1936)
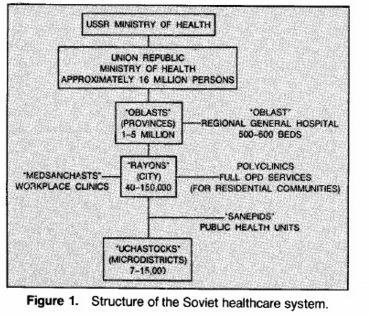
The system itself, known as the Semashko system (in comparison to the Bismarck and Beveridge models of welfare states) is described below in some of the articles I reference. Overall, it was centrally planned, and had a tiered, hierarchical structure. It was free for every citizen. Two of its most remarkable features, that have been widely cited by nonexperts as proof that the Soviet system worked are the high number of hospital beds, and the high number of physicians.These, however, are not measures of effectiveness (outputs), but of costs (inputs). Healthcare systems are to be judged by the outcomes they produce, relative to the resources they use, not by the resources they use alone.
It will be argued in this post that the system had a poor performance, and was inefficient . Besides improvements in health conditions in the 20s-50s, the system was stagnant from there to the demise of the Soviet Union. In the 80s, attempts were made to decentralise the system to make it more flexible, without much success.
In this post, I don't cover the post-Soviet Union period. Seehere and here and here and here andhere for how the current post-Soviet system works.
Overall assessment
The first source we will examine is aCIA report from 1985, released in 1999 to the public. Surely this hardly counts as the last word on the matter, for it is plausible to suppose that the CIA is not the most ubiased source regarding Soviet matters. Or maybe it is, if US policymakers required accurate information precisely to gauge their cold war rival accurately. We will review lots of papers in this post, so we need not worry about this.
The report is highly critical of the Soviet system in general, highlighting underfunded healthcare, lacking qualified personnel, and prevalent shortages of supplies. In terms of outcomes, the system was not able to stop increasing mortality and decreasing life expectancy. The healthcare system for high ranking party members, however, offered better quality.
Some few legal fee-for-service clinics existed, and were heavily used to access better healthcare. Bribes for the same purpose were also common.
 Source: CIA report
Source: CIA report
The Soviet system was apparently focused on curing, not on prevention. Typhoid fever rate in 1979 was 30 times the US ones, and measles rate was 20 times as high. Only 40% of cervical cancer cases in the SU are known before they are terminal, in contrast with 70% in the US. Everything the CIA says is backed by the literature that came after it, so their guesses at the state of Soviet healthcare were fairly accurate.
Early assessments
Friedsenberg (1987) visited Leningrad (modern day St. Petersburg) and interviewed physicians and medical students, visited polyclinics and asked people about their experience with their healthcare system. His report claims only to represent the health system of Leningrad, Soviet Union's second largest city, and so it may be taken as the best the SU had to offer in healthcare.
Polyclinics were medical facilities (for outpatient care) located in neighbourhoods, and people were attended there for free, by a physician that was assigned to them. These facilities served to treat simple problems, provide vaccinations, and do diagnostics. Then, there were regional polyclinics, staffed with specialists, to deal with particular illnesses and were furnished with more advanced equipment. Some equipment like magnetic resonance and computed tomographic imaging devices were almost nonexistant. Advanced medical techniques like 'coronary artery bypass grafting, carotid endarterctomy and angioplasty' also weren't generally available.
Many people reported that they had little confidence in polyclinic physicians, and that they usually visited them to get a work excuse. Medicines were usually imported from outside the SU, but people were able to purchase them at low prices from pharmacies, if they were able to find them, as some of them were in shortage. To reduce costs, some supplies, like needles, gloves, intravenous tubing or catheters were reused in polyclinics. In regional polyclinics, there were waiting lists for elective operations.
Overall, Friedsenberg considers Leningrad's healthcare as "somewhat behind" western standards, but that when compared to its past, the quality was improving, and physicians and people were in general satisfied with it.
Massell (1987) comments on Friedenberg's, and says that he witnessed a vascular surgical procedure in Moscow in 1969 and in 1984. The equipment quality at the centre visited in 1984 was comparable to the United States' best.
Zelicoff (1987) point out that despite Friedenberg's explicit declaration that his article applies just to Leningrad's system, he generalises it to the whole SU in his conclusion. He doubts that is true even in Leningrad itself. He comments on the practice of bribing lowly paid physicians to get adequate treatment.
Also writing in that time, Albrecht & Salmon (1987) confirm the accounts presented before, giving some extra information on how the Soviet system was structured. They suggest their emergency assistance service, was exemplary, highlighting that ambulances were able to reach most citizens in just around 15 minutes. Every citizen had access to "reasonable quality care". This is the only author that praises the emergency system, but I personally doubt his claims are valid for most citizens in the SU, though perhaps they were true for larger cities.
 Source: Albercht & Salmon (1987)
Source: Albercht & Salmon (1987)
They also mention that there were differences in the quality of healthcare provided: those high in the Communist Party hierarchy had access to better services, and that some people bribed physicians to access better care.
Regarding the low cost of the Soviet system, they explain it by several factors: low salaries, less diagnostic tests, less advanced equipment and less expensive end-stage operations. In contrast, the Soviet system had longer lengths of stay in hospitals, and more doctor visits.
Raferty & Schultz (1988) comment on Friedenberg's article, saying that the Soviet system was even worse than he described, with rising infant and overall mortality rates, and prevalent technological backwardness that resulted. Poor quality, corruption, and bribes to have operations done were widespread.
Gananian (1988) comment on Rafeirty & Schultz's comment on Friedenberg's article. He worked some time in Georgia, while Rafferty & Schultz served in Kiev and Rostov. Like Raferty & Schultz, Gananian thinks the Soviet healthcare system was worse than Friedsenberg think it was.
Later assessments
Bernstein & Shuval (1994) provide an evaluation of the Soviet healtcare system by means of asking a thousand of soviet Jewish physicians who inmigrated to Israel in 1990.
The article opens by saying that during the past 20 years, the health of the population in the SU has declined. Infant mortality first declined from 35.3 per 1000 births (1960) to 22.9 (1971), but then increased to 31.1 (1976). It then dropped again, and rose again to 25.4 (1989). This figures are two or three times higher than other industrialised nations. Life expectancy dropped from 67 (1964) to 63 (1980s), and then it increased to 65 (1987), compared to 71.5 in the US, 72.7 in Italy, 74.2 in Sweden, and 75.5 in Japan. Healthcare spending decreased from 6.5% of GDP (1965) to 6% (1970s) to 4.5% (1985) to 4% (1987), making the SU one of the countries that invested the least in healthcare.
This decline was recognised by E.N. Chazov, late Soviet Minister of Health (1987-1990), who complained about the lack of funding for healthcare. In rural areas, only 35% of hospitals had hot water, 27% had no sewage system, and 17% had no running water. The Council of Ministers answered by promising to double healthcare spending by the year 2000, and introduce private enterprise in the healthcare system.
The SU had the highest physician-patient ratio in the world (42 per 10000 population), compared to 13 in the UK, 19 in the US, 24 in Denmark and Sweden. But according to Chazov, this need not be an indicator of quality: many of medical school graduates were not able to, for example, read an electrocardiogram.
Soviet physicians received little pay for their work: 82% of average wages (1965), and this amount declined to 70% (1985) of what an industrial worker made. Gorbachev raised their salaries 30-35%. In 1960, 76% of physicians were women, but active measures were taken to recruit more men into medicine, lowereting the number to 66%. However, lower-ranking positions, like primary care, were still mostly staffed by women (88%).
Out of the interviewed Jewish physicians, 98% were specialists, with half of them having two fields of specialisation. 85% of specialists became so via 3-6 month courses.
Most (90%) of them reported being dissatisfied with the drugs available to them, 84% were disattisfied with the availability of medical equipment, and 75% were dissatisfied with their salaries. During the perestroika era, these indicators didn't improve, or worsened in some cases.
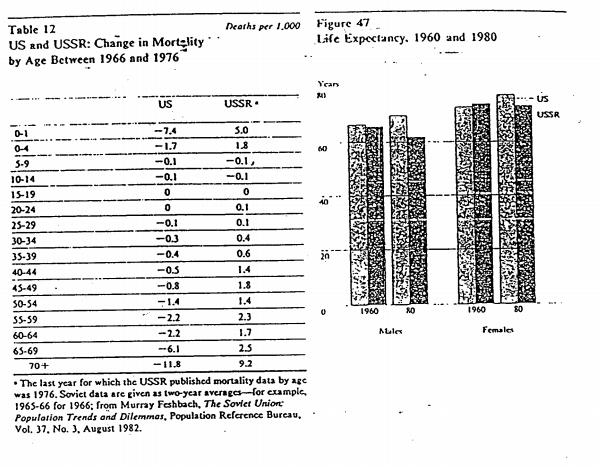
Rowland & Telyukov (1991) again confirm the statistics mentioned before: poor life expectancy, high mortality rates, underfunding (3.4% of GDP vs 11.4% for US in 1989), antiquated facilities, old equipment, low morale, and dissatisfaction. High inequality in healthcare quality existed between individual republics, and between rural and urban areas.
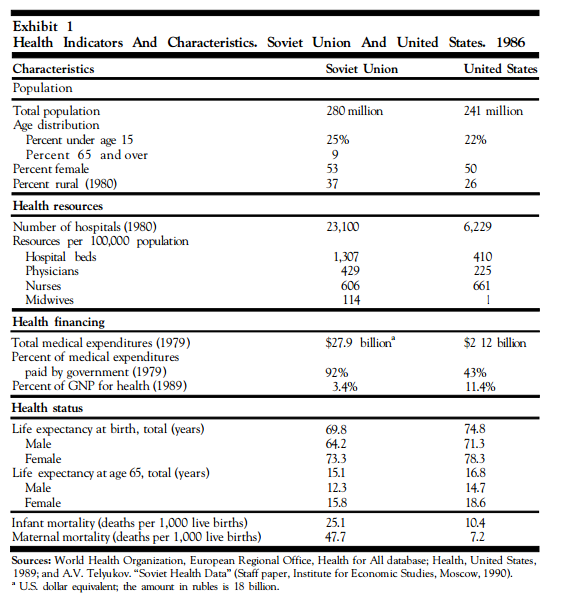 Source: Rowland & Telyukov (1991)
Source: Rowland & Telyukov (1991)
This happened even when the Soviet Union had larger numbers of health personnel (twice per capita as the US), number of hospital beds (three times per capita as the US), and facilities.
For most causes, mortality rates were higher in the SU than the US in 1988,
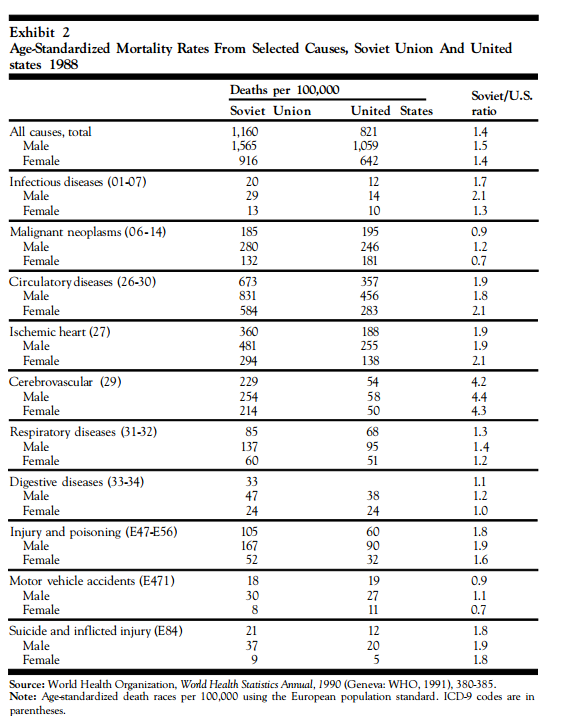 Source: Rowland & Telyukov (1991)
Source: Rowland & Telyukov (1991)
Life expectancy not only was lower in the SU, but for females it was virtually stagnant, and for males it actually declined 1958-1978, to rebound again to its previous peak.
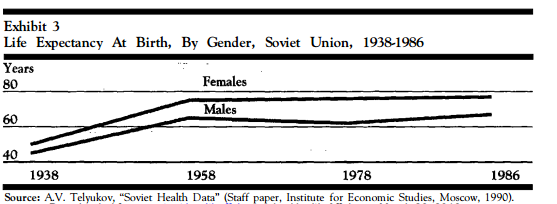 Source: Rowland & Telyukov (1991)
Source: Rowland & Telyukov (1991)
Some reasons for this, besides the poor quality of the system, are a high number of smokers and alcoholics, low levels of physical fitness, poor diet, and a having a sizable (15%) fraction of the population living in areas with pollution 10 times higher than 'normal' levels.
The soviets were aware of this deficiencies (in part, due to the glasnost [openness] policy) and were trying to implement some measures to fix the system. These measures included devolving control of healthcare to the individual republics instead of having SU-wide control, relying on state-enterprises to provide healthcare in the workplace, and experiment with health insurance. Hospitals would be communitarized, or privatised to communities: instead of being government-owned, they would be nonprofits run by local communities. Other ideas were to copy the US HMO system, and reward competence and productivity to motivate physicians. Overall, the idea was to decentralise the system.
Schultz & Rafferty (1990) describe the state of soviet healthcare, and Gorbachev's plans for reform in the perestroika period. They are in agreement with the authors above.
Contrary to its stated principles,'0 the Soviet medical care system is neither unified nor egalitarian. Most people get care in hospitals and clinics operated and funded by the Ministry of Health, a system of free care that includes 94 percent of all health care facilities. A parallel "closed" system is maintained by certain elite government ministries and by large factories. This "closed" system is considered to be of higher quality than the "public" one and draws a disproportionate share of all health funding. Doctors find work in this system attractive; half of all doctors in Moscow work in just 30 "closed" clinics where their workload is lighter and their pay higher than that of doctors in the public system.
Also contrary to its design, Soviet health care is not free. Patients treated in the public system are often required to pay doctors and nurses under the table in order to assure that medications be administered or that an operation be performed. A Soviet newspaper recently published some sample "prices": 500 rubles for an operation or delivery (the average monthly salary in the USSR is 200 rubles), 300 rubles for a 20-day hospital stay, 25 rubles or the donation of a unit of blood by a relative to assure admission to the hospital. Most patients must purchase medications and appliances at prices that include "surcharges" demanded by sellers who manage to overcome bureaucratic obstacles and short supplies.
[...]
The results of these developments are most obvious in the lack of technological sophistication of medical care in the USSR. For example, by Soviet estimates, there are about 50 computerized tomographic (CT) scanners in the entire country, or less than 2 percent of the US per capita number.15 Many of these scanners are Soviet-made, have limited capabilities, and are in operation an average of only five to six hours per day because of technical and organizational problems.' In Kiev, the fourth largest city in the USSR, we were told that there was only one operational CT scanner and two obstetric ultrasound machines for a metropolitan area population of some three million. At a national oncology center we were told that Papanicolaou staining often could not be done due to lack of materials and that a pH-meter was the only "automated" blood analyzer. On an ambulance run, we waited 90 minutes to use the only functioning electrocardiograph available that night to the emergency medical teams serving approximately one-third of Kiev. In Moscow, a surgical intern reported that he is limited to ordering six laboratory tests three times weekly. Disposable equipment is rare, and most equipment is scarce. For example, paramedics we accompanied on urban ambulance runs were rationed two to three reusable hypodermic needles and one syringe, necessitating mixing of medications before infusing. This practice is apparently common, judging from wall charts of miscible medications we saw on hospital wards. Drugs, especially antibiotics and cardiovascular preparations, are in short supply, of poor quality, and archaic. For example, a 1987 textbook of internal medicine suggests the use of leeches to treat malignant hypertension
We were struck by the low intensity of care on medical and surgical wards in tertiary care teaching hospitals, particularly the lack of nurses and monitoring equipment. The Minister of Health has acknowledged that many hospitals are "little more than places to sleep," and lengths of stay average 17-18 days as patients await diagnostic studies utilizing outdated, broken, or inefficient equipment.Countrywide, 40 percent of hospital beds are in buildings originally constructed for other purposes, and rural hospitals often lack hot water and sewage.
The outlook for containing the spread of human immunodeficiency virus (HIV) in the USSR is bleak. The reported number of HIV-infected Soviet citizens reached 292 in July 1989, 40 percent of whom were infected by transfusion of blood during surgery.24 Eighty-one other cases have been traced to pediatric wards in three cities where the virus was spread from child to child through the reuse of unsterilized equipment. Some of these children were referred to other, more specialized hospitals, where the virus was spread further.25 The Soviets plan to test 35 million blood samples26 for HIV in 1989-testing blood donors, pregnant women, foreigners, and Soviets who travel abroad. Until now, however, because of a shortage of testing materials27 some of these tests have been performed on pooled, mixed sera from several patients.
Changes proposed:
Like all aspects of the Soviet economy, health care is planned and directed centrally. The architects ofperestroika hope to decentralize economic decision-making by the introduction of a system of individual incentives and penalties throughout the economy, including the health sector. Economic reform movements are nothing new in the Soviet Union, but the scope of the current effort and the magnitude of the problems faced by the Soviet economy are unprecedented. The basic principles of perestroika were laid out in June 1987 and the specific proposals about health two months later, in August 1987.
In general, health care will be entitled to a greater share of the gross national product and local officials will assume greater fiscal responsibility for the way the system functions. There are some specific provisions designed to promote the limited spread of patient-paid care, the further development of technology and its incorporation into practice, and an emphasis on preventive care. The proposed changes are quite striking, but as with many previous attempts to improve the lot of the average Soviet citizen, there are many political, economic, and social factors that may limit the success of this latest endeavor. The leadership has made a commitment to increasing the share of the gross national product that goes to health from 3.9 percent to 6 percent by the year 2000.
A second focus is to be a re-emphasis on prevention (dispanserizatsia in Russian). Preventive medicine and periodic health examinations have been a cornerstone of official Soviet health policy since the Revolution, although in practice the required physical examinations have been done perfunctorily or not at all.2 Initially children, war veterans, pregnant women, and farm workers will be required to undergo annual checkups beginning in 1991, and the rest of the population will be examined after 1996. In contrast to screening methods employed in the United States, which are targeted by age- and disease-specific risk, dispanserizatsia has been a wasteful and unsuccessful program which currently includes such practices as using fluoroscopy as a screening procedure for pulmonary tuberculosis.
A fundamental reform, the gradual introduction of private enterprise in the form of cooperatives (a Soviet euphemism for private business), is taking place in health care as well as in the general Soviet economy. Staff-owned medical cooperative clinics and even a recently opened homeopathic hospital [ndE: Homeopathy, acupuncture, and 'tradicional medicine' also existed in the Soviet Union]37 are to rely solely on patient fees to cover operating expenses, drawing no state funds but returning profits to their owners and staff as income. These will supplement the volume of for-pay medical services already provided in state-owned "self-financing" clinics which receive some state funding but are not privately owned. Many people prefer to pay for services in these clinics, reflecting a prevalent Soviet belief that "you get what you pay for in medical care." In Moscow, where 20 of these clinics are located, 2.7 million of 126 million ambulatory visits in 1986 took place in these "self-financing" clinics.
The process of regulating cooperative clinics has just begun. In late 1988, cooperatives were prohibited from using or paying for the use of state-owned diagnostic equipment39 and, more recently, the government barred cooperatives from many medical activities. The list of prohibitions includes:
treating and evaluating severely ill psychiatric patients;
treating cancers, drug addiction, occupational illnesses, infectious and especially sexually transmitted diseases;
providing obstetric care or abortions,
any form of surgery;
use of invasive diagnostic methods; and
production of medications, including narcotics.
Although legal, moonlighting activity by physicians in the past was heavily taxed and regulated (and largely unreported). It provided an estimated six to eight times the volume of services up to now provided in "self-financing" (patient paid) clinics, and 74 percent of the population acknowledge paying for the services of moonlighting physicians.4" Under the new system, doctors must continue to work in a full-time position in a state-run facility, and they will be allowed to earn no more than 140 percent of their base pay. A system of fee-for-service payment for nurses is being introduced as well
It is not clear that the government has the means to finance an expansion in health spending. The anti-alcohol campaign, recently de-emphasized, may compromise the government's ability to fund other improvements in health. Since the price of vodka was doubled and the hours of operation of stores that sell alcohol were shortened in 1985 the decline in sales has created a 10.4 billion ruble shortfall in government revenue. (The entire state budget for health in 1985 amounted to just 17.6 billion rubles.8) The loss of this revenue, along with a recently announced 36.3 billion ruble budget deficit in 1988, may prevent the government from instituting its own health budget increases.44 Improved performance in the rest of the economy as a result ofperestroika (the Soviet government does collect taxes) and announced reductions in military spending might increase funds for health care, but such improvement is not likely to materialize for several years. Without better matching of supply and demand than is now achieved, even unlimited funding for health care cannot assure an adequate supply of medical manpower or materials for purchase. Even now, funds allocated for health are often returned to the treasury unspent. [...]
There is much popular skepticism (still expressed privately) about perestroika,49 and many Soviets we asked expressed skepticism about the leadership's commitment to reform health care in particular, since the bureaucrats and party bosses, sheltered by a network of exclusive clinics and hospitals, have not suffered the consequences of their mnattention to the public system. The failure of Gorbachev's first program directed at health, the 1985 campaign against alcoholism,8 has increased suspicion that government planners are not capable of organizing successful health care programs. In conclusion, the resolution of the current economic crisis in the Soviet Union will determine its relevance as a world economic power into the twenty-first century. There is a crisis in the health sector, too; the record of declining health indices, the lack of technological sophistication, and the poor quality of medical care are well known in the West. We have added our own observations about that record and speculate that because of inadequate funding, scant access to Western capital, and constraints placed on the development of alternatives to the state health care system, real improvements in this area may not appear soon. A year after the announcement of plans to reform the Soviet health care system, Chazov challenged the timidity of the reforms at a special Communist Party conference: "If we (the Soviet Government) truly want to resolve the problems of health care, we must immediately change the standards by which that care is planned and financed." Future improvements in the general Soviet economy and greater administrative flexibility will determine whether the Soviet health care system will improve.
Field (1990) is somewhat less harsh in his critique than Rafferty and Schultz, but he is far from praising its achievements.
The infant mortality debate
Davis (2006) reviews Eberstandt's (1981) article on increasing infant mortality in the SU in the 70s. This article challenged the prevailing conceptions that the socialist countries were improving the health of their populations and that they were models for others to imitate. He explains the state of the debate in the initial years:
In the late 1970s the USSR was considered to be a successful and expanding world power, whereas the West was on the defensive (e.g. economic ‘stagflation’ following the 1974 OPEC embargo, defeat of the USA in Vietnam, socialist revolutions in Africa, growing Soviet military power). Many in both the East and West considered that the ‘correlation of forces’ was in favour of the socialist bloc and its Third World allies. [...]
The objective study of health in the USSR was seriously impeded by the comprehensive and reasonably effective Soviet censorship system. In the case of mortality rates, during 1955–71 the Soviet Union published the infant mortality rate (but not perinatal, neonatal, and post-neonatal rates), the crude death rate, age-specific death rates, and life expectancy at birth in its annual statistical yearbook, Narodnoe Khozyaistvo SSSR (there were no electronic databases in those days). Maternal death rates (quite high) were published only sporadically in specialist journals. In response to the deterioration in the health situation, the USSR ceased publication of life expectancy after 1972, infant mortality after 1974 and age-specific death rates after 1976. Soviet specialists used a unique and misleading methodology to calculate infant mortality (high risk live births were excluded from consideration), which underestimated the actual rate by 14.4%
Although demographic and health specialists in the Soviet Union produced thousands of studies in Russian and other USSR languages on the health situation, and a number of these scholars were first rate, their access to accurate statistics was restricted by the government and the censorship system (state control of all publications) limited their ability to call attention to serious problems and prohibited them from suggesting that there were systemic causes of any difficulties. Soviet-Western academic cooperation was extremely difficult.
Studies by Western specialists were constrained by the facts that few of them possessed knowledge of Russian language and that the Soviet Union published only a small amount of information in Western languages. The USSR provided minimal quantities of demographic and health statistics to the UN (for the Demographic Yearbook) and the World Health Organization (but nothing to the World Bank and OECD). All WHO publications related to health in the USSR were either prepared by Soviet specialists or vetted by Soviet authorities, and contained even less critical analysis than that found in Russian language sources. Official Soviet books on health published in foreign languages provided some useful basic information, but essentially were propaganda documents. [...]
Overall, the situation with respect to health in the USSR in the 1970s had some similarities to that outlined by Kuhn in The Structure of Scientific Revolutions. A ‘normal science’ concerning health in the USSR existed that was accepted as truth by most concerned parties and offered what appeared to be a reasonable explanation of reality. Certain anomalies had arisen, notably rising mortality rates, that posed questions about the prevailing paradigm, but no crisis was perceived to exist in it and there was little pressure for a paradigm shift. [...]
Over the next several years the general findings that mortality really had risen in the USSR and that serious health problems existed there became widely accepted in the West and a component of a new paradigm that interpreted the Soviet Union as a failing system. However, several serious articles challenged our analyses. Jones and Grupp observed that the growing awareness of the upward trends in mortality in the USSR resulting from the Davis–Feshbach and Eberstadt publications ‘has contributed to an abrupt reversal of Western perceptions of Soviet medicine and its system of health care’. They argued in their conclusions that this negative assessment was unwarranted because ‘it is clear that much of the highly publicized increase in reported rates between 1971 and 1974 reflected improved vital registration, not a deterioration of the medical system or of maternal and child health conditions’. A demographic study by Anderson and Silver concluded that ‘the evidence for a real increase in infant mortality in the Soviet Union since 1971 is weak’. In contrast, Mark Field, a renowned specialist on Soviet health, argued with respect to the rise in infant mortality that ‘we must assume that from one half to three quarters was real’. [...]
The responses to the Davis–Feshbach report and Eberstadt article in the USSR were mixed. In the first half of the 1980s there was a tightening of Soviet censorship in the health field in an attempt to keep a lid on the story of deteriorating health. The official attitude toward our findings was quite critical and several Soviet publications took issue with them. The most detailed critique was published in Anitsovetizm Burzhuaznoi Demografii (The Anti-Sovietism of Bourgeois Demography).According to it, the Davis–Feshbach report was ‘exceedingly tendentious in its essence, but had the appearance of scientific objectivity’. Both of the publications were ‘a fundamental part of the anti-Soviet campaign, directed toward the ideological preparation of the population of the USA for the cold war’. At the unofficial level, there was considerable interest in our work and Murray and I received some favourable feedback during our trips to the USSR.
Following Gorbachev's accession to power in 1985 the Communist Party line changed substantially. The previous decade became known as the ‘era of stagnation’ and many acute social problems associated with it were identified, including rising mortality, as a result of the new policy ofglasnost' (openness). The official publication of mortality and life expectancy statistics resumed, reforms were introduced to correct problems in the health sphere, and mortality rates temporarily declined.
McKee (2006) presents a similar view.
Mortality rates and life expectancy
Kumo (2013) surveys research on mortality trends and other indicators in Russia. Regarding lif expectancy, a figure summarises trends from 1961 to the end of the SU:
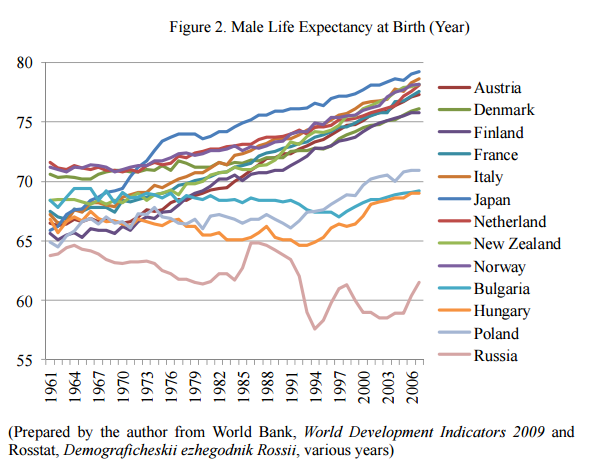 Source: Kumo (2013)
Source: Kumo (2013)
The increase in life expectancy in the 80s was, according to the author, to Gorbachev's anti-alcohol campaign.
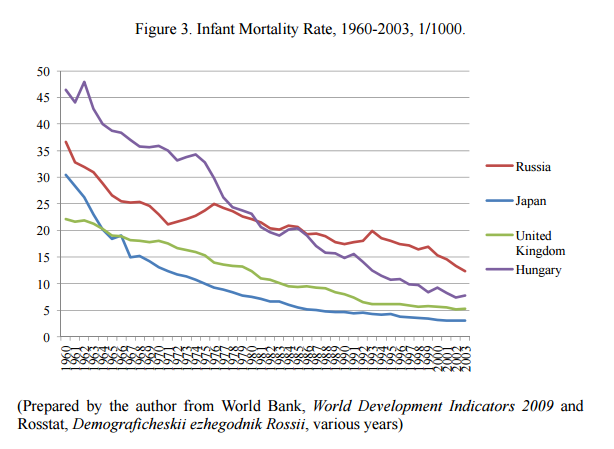 Source: Kumo (2013)
Source: Kumo (2013)
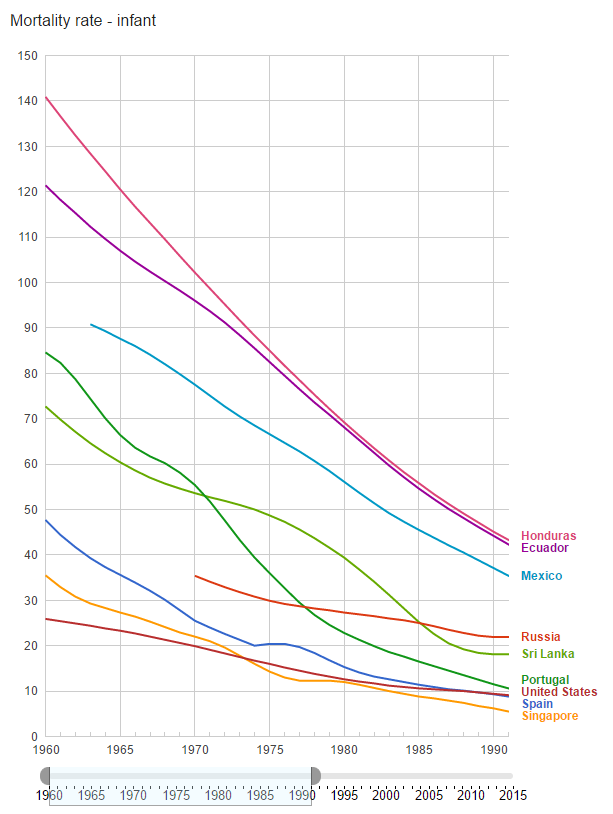
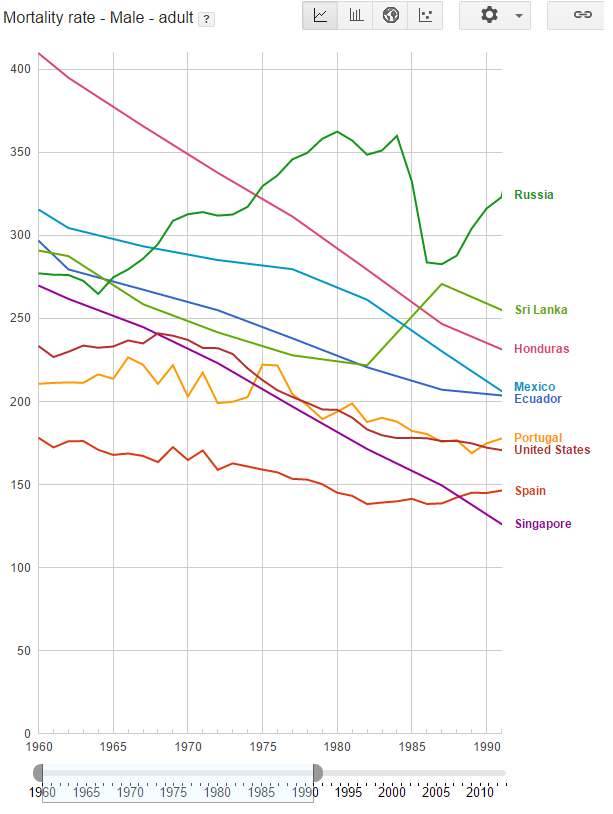
We can make the comparison clearer by using the same countries that back in 1922 had the same GDP per capita as the Soviet Union,
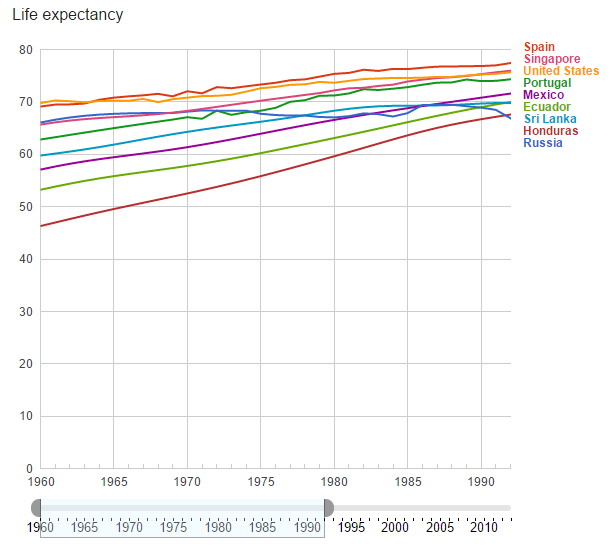 Source: World Bank
Source: World Bank
 Source: World bank
Source: World bank
 Source: World Bank
Source: World Bank
If we assume that the life expectancies were equal in 1922, something that is perhaps too much of a stretch, we could say the Soviet system did initially better than the one in Honduras, Ecuador, Mexico, and Portugal, and as equally good as Singapore's. Spain did better. The US is there for comparison. But in the period depicted here, stagnation ensured that all those countries ended up surpassing Russia. Russia was not the Soviet Union, but roughly half of the SU population was there.
Kumo comments on the high number of hospital beds and doctors,
In the Soviet Union medical services were provided for free, and in terms of quantitative indicators such as the number of doctors, nurses, and hospital beds, the level of medical care was superior to that of developed nations. This much is widely known, and can also be seen in official statistics from the Soviet era (Levin, 1979; Kotryarskaya, 1990; Cromley and Craumer, 1990, 1992). From the Soviet era to the present day, the number of doctors and nurses has been high compared with developed nations. In 1985, during the Soviet era, there were 3.9 doctors for every 1,000 people7 . In the same year in the U.S., there were 1.7, while in Japan the figure was 1.5. Even in 2000, Russia had 4.2 doctors for every 1,000 people, a figure that was only surpassed by Greece (with 4.3) among the OECD nations.
He then says that the rise in mortality rates were not due to worsening healthcare or increases in pollution, but to increased levels of alcoholism. However, he doesn't cite much evidence to support these claims. For healthcare, he says that it's not plausible that heealthcare deteriorated if there was economic growth until the 80s, and that in 1961, Japan was able to import 10 million vaccines for polio from the SU. This is inconsistent with the picture the other researchers show, both qualitatively and quantitatively: even if there was growth, healthcare spending went down. And then, it is possible for quality to go down as spending is constant.
Anthropometric data
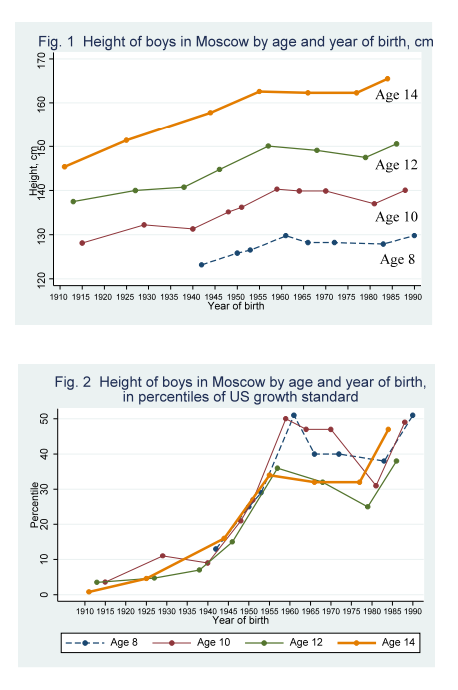
Brainerd (2008) studies anthropometric data, and concludes that initially, the rate of growth in children height compared favourably to that of similarly developed nations in the pre-1970 period, stagnating afterwards.
Data for 14-year olds cannot rule out the hypothesis that this growth rates were just continuations of the trends present in the Russian Empire.
 Source: Brainerd (2008)
Source: Brainerd (2008)
She concludes
While the Soviet experiment of the twentieth century clearly failed and in countless ways harmed the lives of Soviet citizens, the record of Soviet health achievement prior to 1970 remains impressive.
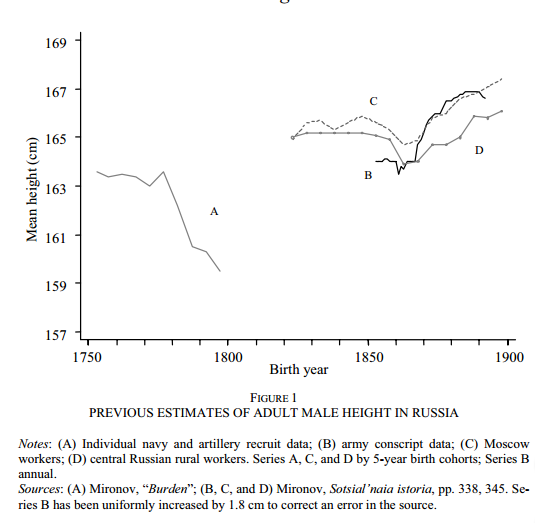
Mironov & A'Hearn (2008)study anthropometric evidence from the Saratov province region in the tsarist era. The first provide previous estimates
 Source: Miranov & A'Hearn (2008)
Source: Miranov & A'Hearn (2008)
They then introduce new measurements from the Saratov province,
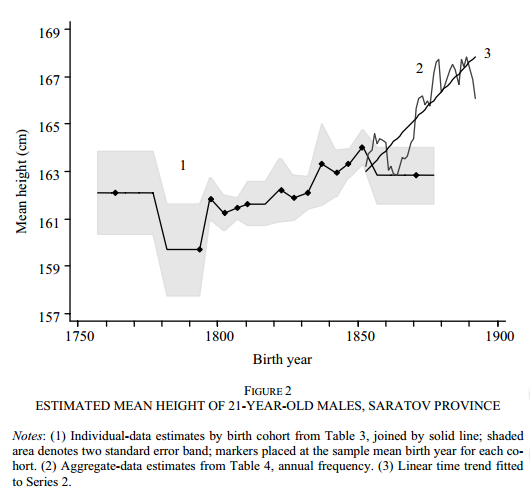 Source: Miranov & A'Hearn (2008)
Source: Miranov & A'Hearn (2008)
This confirms the rising trends present in the Russian Empire, therefore giving more plausibility to the thesis that height increase in the early SU was a continuation of previous trends.
In a recent review of heights and their relation to health, by Steckel (2009)mentions work by Komlos (1999), who argues that improvements in health in Russia (as measured by height) were not particularly good, not only after 1960, but even before, in comparison with Mexico, Philippines, Spain, Chile or Jamaica.
(EDIT)
In 1984, Mark G. Field published some brief notes as part of a conference report about the quality of life in the Soviet Union.
It is difficult to speak of the quality of life in the Soviet Union without discussing the Soviet health care system. There is no doubt that the principle of free and universally accessible medical service as pioneered by the Soviet Union is heartily endorsed by the Soviet population. This principle derives from the idea that healthcare is such an indispensable aspect of the quality of life that (like education) it cannot be left to the vagaries of the marketplace. In principle, it guarantees every Soviet citizen the full gamut of clinical and preventive services at the expense of society. In reality, however, if one is to judge from the testimony of outside observers and Soviet sources themselves, the system is but a pale reflection of what it is meant to be.
It is ironic that a new society whose great ideological appeal is equality should have spawned a multi-class medical system. In the health field, Soviet propaganda initially promised the elimination of first- and second-class medical systems as they existed under the Tsars. But ever since the early days of the Revolution, this has not been the case, as those who governed received special medical attention and rations. The si tua ti on became even more polarized during the 1930s as a result of Stalin's deliberate policies to eliminate egalitarianism as left-wing or infantile deviation. Soviet society has given rise to an elaborate system of rankings and distinctions, which are followed quite closely in the provision of medical services. The health care system in the Soviet Union is divided, broadly speaking, in to two unequal categories : territori a 1 networks and closed networks. Territorial networks serve the general population and are accessible by virtue of residence. Closed networks, on the. other hand, are reserved for special groups.
At the lowest level, there are facilities reserved for workers of industries with over a certain number of personnel. Next, there are special facilities for certain agencies of ministries, such as the armed forces, or the Ministry of Internal Affairs. Another network is reserved for intellectual elites, such as members of the Academy of Sciences or leading artists. Finally, at the apex of the Soviet medical (and socio-political) pyramid is the network of medical institutions and rest homes, etc., reserved for the Kremlin elite and their families. This network of high-quality medical care parallels the other perquisites of rank, such as private dachas, chauffeured limousines, restricted special stores, and so on. This is sometimes reffered to as the Fourth Administration of the Ministry of Health Protection.
Just as there are special detention centers in all Soviet cities, there are also specialized clinics and hospitals where the elites can receive medical care far removed from the scrutiny of the c0fl11lon man. These facilities may be free standing or merely restricted sections of general hospitals. The major difference between these facilities and private rooms in American or British hospitals is that members of the Soviet establishment do not pay for their privileged treatment. The Soviet elite receives medical care as a perquisite of rank, paid by the state--paid for in fact by the taxes of ordinary citizens who must content themselves with ordinary hospitals and clinics. Needless to say, medical facilities reserved for the elites are better equipped that those in the ordinary networks.
According to the observations of William Knaus, M.D., equipment, drugs and procedures not available in the Soviet Union are imported from abroad, either from Eastern Europe or the West if necessary. In some instances, top specialists are invited to come to the Soviet Union to consult on important cases or operate.
The Soviet press repeatedly reports complaints received by readers about the rigidities of the medical system. Hospitals;, for example, will not admit new patients after a specified time of day. Every disease is. tariffed according to the number of hospitalization days it is permitted. A delivery is usually nine days; an appendectany is ten days. Even if the patient is well enough to be discharged earlier, this is not allowed. Patients will be subjected to routinized procedures whether they need them or not. Bureaucratically determined rules overload physicians in outpatient clinics, thus reducing the time available for those who really need a doctor. While meaningless rules are enforced as to what one can bring into a hospital, sterility is poorly observed in operating rooms. As a result, the incidence of post-operative infections is very high, affecting about one-third of all patients operated on. The rigidities of the Soviet health care system is epitanized by the extensive use of quotas. Hospitals are assigned "death quotas," and investigations will follow if they exceed these quotas. The result is that hospitals often refuse to admit terminally ill patients, placing the burden entirely on their families. There are also quotas for all types of operations and hospital occupancy rates. The result in this case is the widespread tendency to falsify records and statistics. Hospitalization quotas are almost always met in the Soviet Union--at least on paper--because if they were not fulfilled, budgets and supplies might be curtailed in the next fiscal year. Thus the hospital manager plays the same game as the industrial manager. It is not unusual, nor seen as improper, to request twice as many supplies as needed since the director knows that he will be lucky to get half of what he requests. [...]
Given the fact that the health care system is not a high priority area in the Soviet economy, it suffers the same shortages and erratic distribution patterns as the rest of the economy. A review of Soviet materials reveals an extremely inefficient system, riddled by bureaucracy, poor quality and severe problems of production and distribution. Shortages of medical supplies are chronic, and the system works poorly to inform physicians of new medical products and techniques. Although drug retail prices are very low, the patient is often unable to obtain prescription and non-prescription items, or only with great difficulty.
With its plethora of physicians and hospital beds, the Soviet medicine system seems impressive at first glance. But indeed, in some instances, it resembles the medical systems one sees in lesser developed nations. The level of infant mortality is certainly not what one might expect of a highly industrialized nation with an economy second in size only to the United States. With the exception of the elites, the population in general receives a kind of mass medical care which pays scant attention to detail, quality or the personal feelings of patients. Improvements in the quality of the Soviet health care system will require important changes in structure, attitudes of health personnel, and significantly higher budget allocations. But if the medical industry does produce certain goods, more money will not necessarily help. The problems of the Soviet medical system ~re representative of the problems of Soviet society in general, and the solution to the former are not possible without solutions to latter.
Conclusion
The Soviet healthcare system heavily underperformed most of the countries that we can use as meaningful comparators. Relative to other countries that began from the same situation o poverty as the SU, its performance wasn't better than the systems of those countries. After the 70s, health outcomes deteriorated, and the utter failure of the system became apparent.
Despite the high number of hospital beds and physicians, the Soviet Union wasn't able to deliver better healthcare outcomes to its population, relative to developed countries, even though they made great improvements in the 20-50s era. This should make us wary of making hasty comparisons based just in some indicators instead of considering the bigger picture.
EDIT: Read also this article.
EDIT2: There are some papers that say life expectancy increased a lot in the Soviet transition. For example, this. If true, it would not undermine the account here, for I remarked that the system worked relatively well at the beginning, but broke down later on. However, there are reasons to doubt the accuracy of these measurements. The leading database of life expectancies, The Human Mortality Database (Shkolnikov, Barbieri & Wilmoth) only has data for Russia in the 1959-2014 period, saying that the quality of the data in the period 1959-1969 is lower, and that it should be used with caution. On the other hand, Shkolnikov does give data for the 1896-1959 period in the link in EDIT. Even given this, my conclusion still stands.
References
Albrecht, G. L., & Salmon, J. W. (1986). Anomalies in Soviet healthcare. The Journal of medical practice management: MPM, 2(4), 288-296.
Bernstein, J. H., & Shuval, J. T. (1994). Emigrant physicians evaluate the health care system of the former Soviet Union. Medical care, 141-149.
Brainerd, E. (2010). Reassessing The standard of living in the Soviet Union: an analysis using archival and anthropometric data. The Journal of Economic History, 70(01), 83-117.
CIA (1985), A Comparison of the US and Soviet Economies: Evaluating the Performance of the Soviet System .
Ellison, H. J., Johnson, B. P., & Raynes, E. A. (1984). The Quality of Life in the Soviet Union: A Conference Report. Kennan Institute for Advanced Russian Studies, Woodrow Wilson International Center for Scholars.
Field, M.G. (1984) Medical care in the Soviet Union: Promises and Reality (in The Quality of Life in the Soviet Union: A Conference Report, ed. H.J. Ellison et al.)
Field, M. G. (1990). Noble purpose, grand design, flawed execution, mixed results: Soviet socialized medicine after seventy years. American Journal of Public Health, 80(2), 144-145.
Friedenberg, D. S. (1987). Soviet health care system. Western Journal of Medicine, 147(2), 214.
Gananian, M. (1988). Deficiencies in Soviet Medicine. Western Journal of Medicine, 149(2), 225.
Komlos, J. (1999). On the biological standard of living in Russia and the Soviet Union. Slavic Review,58(1), 71-79.
McKee, M. (2006). Commentary: The health crisis in the USSR: looking behind the facade. International Journal of Epidemiology, 35(6), 1398-1399.
Massell, T. B. (1987). Soviet health care. Western Journal of Medicine, 147(4), 475.
Mironov, B., & A'Hearn, Brian (2008). Russian living standards under the tsars: anthropometric evidence from the Volga. Journal of Economic History, 68(03), 900-929.
Rafferty, M., & Schultz, D. (1988). Medicine in the USSR. Western Journal of Medicine, 148(5), 585.
Rowland, D., & Telyukov, A. V. (1991). Soviet health care from two perspectives. Health affairs, 10(3), 71-86.
Steckel, R. H. (2009). Heights and human welfare: Recent developments and new directions.Explorations in Economic History, 46(1), 1-23.
Zelicoff, A. P. (1987). Soviet medicine. Western Journal of Medicine, 147(5), 598.
Comments from WordPress
- On the express acceptance and rejection of beliefs | Nintil 2016-04-10T11:53:19Z
[…] recently wondered how the Soviet healthcare system worked. Initially, I thought, based on broad ideas about the USSR, that it wouldn’t work very well. […]
Oleh Kravets 2016-08-02T20:52:19Z
According to my mother, hospitals in the 80th's were really shitty even in comparison to those in the modern Ukraine. The qualification of personnel has worsened though, mainly because of drastically increased corruption in the education system.
- The Soviet Union series | Nintil 2016-05-14T15:56:57Z
[…] The Soviet Union: Healthcare […]
Midofe 2016-07-14T21:22:34Z
Gran post, no tienes alguno sobre el sistema educativo soviético? es cierto que los soviéticos tenían mas universitarios y científicos que Estados Unidos?
Artir 2016-07-14T22:06:15Z
Tengo uno pendiente sobre ello, ya llegaré. Ahora ando ocupado con otros temas.
Comments